Painless heart attack
Normally
when
blood
supply
to
a
portion
of
the
heart
muscle
is
inadequate
(ischaemia)
you
will
suffer from angina characterised by one of the following -
•
Acute Chest pain
•
Feeling tight in your chest
•
Pain radiating to your left arm, shoulder or neck
If
the
blood
supply
is
cut
off
completely
you
will
suffer
a
heart
attack.
These
symptoms
are
well
known to most of us and we will seek urgent medical help if it occurs.
However,
there
are
many
in
the
world
who
suffer
from
ischemic
episodes
without
realising
it
as
they
do
not
have
symptoms
normally
attributed
to
angina.
This
is
known
as
silent
ischaemia.
They
may
also
suffer
a
heart
attack
with
no
warning.
People
who
have
had
previous
heart
attacks
or
those
with
diabetes
are
especially
at
risk
of
developing
silent
ischemia.
It
is
said
that
"silent"
(asymptomatic)
myocardial
ischemia
is
the
most
common
manifestation
of
coronary
heart
disease (CHD), accounting for more than 75 percent of ischemic episodes during life.
Painless
myocardial
infarctions
on
the
other
hand
vary
a
little
from
silent
ischaemia
or
infarction.
Although
there
may
not
be
chest
pain
or
radiating
pain
in
painless
myocardial
infraction,
other
symptoms relating to the condition may be present. They are:
•
Profuse sweating
•
Palpitation (due to increased sympathetic activity)
•
Breathlessness (due to cardiac failure)
•
Feel faint (syncope due to hypotension)
•
Extreme fatigue (due to poor tissue perfusion)
•
Sometimes patients become unconscious because of
severe cerebral hypoperfusion (not enough blood reaching
the brain).
Both
silent
ischaemia
and
painless
ischaemia
occur
in
poorly
controlled
diabetics
and
non-diabetics
over
the
age
of
seventy.
The
reason
is
because
the
pain
conducting nerve fibres are paralysed in diabetes and old age and hence you do not feel the pain.
If
any
of
the
symptoms
described
above
is
seen,
it
is
essential
to
have
your
heart
checked
urgently. Diabetics must be particularly warned about this.
Investigations:
•
Urgent ECG will normally show changes relating to ischaemia or infarction.
•
Blood
Test
to
check
cardiac
enzymes
and
proteins
should
be
done
even
when
the
ECG
appears normal.
The
blood
test
will
measure
the
levels
of
enzymes
and
proteins
that
are
linked
with
injury
of
the
heart
muscle.
They
include
the
enzyme
creatine
kinase
(CK),
and
the
proteins
troponin
I
(TnI)
and
troponin T (TnT). Their levels will rise if the heart has suffered an injury.
If
the
ECG
and
blood
tests
are
inconclusive
two
further
tests
could
be
done
to
make
sure
your
heart is healthy.
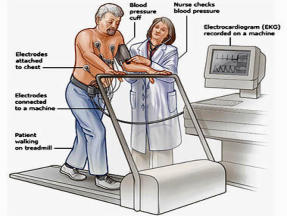
Ambulatory Electrocardiogram:
•
I
f
your
doctor
is
able
to
arrange
this,
a
small
recorder
will
be
attached
by
a
belt
to
your
waist.
The
machine
will
be
connected
by
wires
to
your
chest.
It
will
continuously
record
the
electrical
activity
of
your
heart
as
you
carry
on
with
your
normal
activities
over
a
period
of
24
to
48
hours.
If
your
heart
is
affected
during
this
period
your
doctor
will
be
able
to
pick
this
up
through
the
recording
on
the
machine.
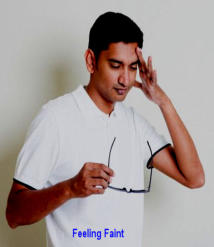
Stress ECG:
•
This
will
be
the
ultimate
test
to
check
if
your
heart
is
normal
and
healthy.
Here
you
will
be
connected
to
the
machine
by
a
few
leads.
The
ECG
is
then
recorded
while
you
are
on
a
treadmill.
The
stress
levels
of
your
heart
will
be
increased
slowly
by
making
you
walk
faster
and
if
necessary with the treadmill at an upward incline.
•
This
test
should
only
be
done
with
a
cardiologist
nearby
as
he
will
know
when
to
stop
the
test
if
you
are
in
trouble
or
will
be
able
to
resuscitate
you
immediately if you suffer from a cardiac episode.
Complication
and
mortality
are
more
often
seen
in
painless
infarction
than
when
you
have
associated
chest
pain.
The
probable
cause
for
high
mortality
is
that
patients
normally
ignore
their
symptoms
when
they
have
no
chest
pain.
They
usually
continue
with
their
routine
activities,
if
symptoms
are
bearable.
Continued
activity
in
the
presence
of
myocardial
infraction
will
lead
to
complications like
irregular
heart
beat,
cardiac
failure
and
death.
This
is
very
common
in
India
compared
to
other
countries.
It
is
estimated
that
more
than
900
Indians
under
the
age
of
30
die
from it everyday.
It
is
more
difficult
to
identify
someone
with
silent
ischemia
or
infarction
as
they
do
not
have
any
symptoms
recognised
as
originating
from
the
heart.
High
risk
populations
(diabetics
and
elderly)
should
be
made
aware
of
this
and
should
be
advised
on
regular
health
checks
and
how
they
should protect their heart.
It
is
important
that
everyone
becomes
aware
of
this
silent
killer.
If
you
have
had
any
of
the
symptoms
mentioned
with
no
accompanied
chest
pain,
do
not
assume
that
your
heart
is
not
the
cause. Seek advice and have your heart checked.
K. Badrinath, F.R.C.S., MSc (Ortho), (Lond)
I would like to thank Prof. S. Vaithinathan, MD., DM Cardiology for his advise on this topic
Madras Red Fort Doctors Foundation
